Although it has been fraught with debate, and even disdain on occasion, the use of airbrushing of photos emanating from the marketing world of skin care and beauty tells us one thing: our society has a desire for evenness in skin appearance.

Acne (or acne vulgaris) is one of the most common skin conditions, affecting 64% of people in their 20s and 43% of people in their 30s. It affects the pilosebaceous units of the skin, which is essentially the oil gland and hair follicle. It usually affects the largest, hormone-responsive sebaceous glands such as those on the face, chest, neck and back.

Itchy skin, dryness, redness, and cracking—uncomfortable signs of an eczema flare-up that can range from mild to having a significant impact on quality of life. Corticosteroid creams can do a fine job of targeting symptoms and inflammation associated with eczema, although below are some suggestions to get to the root cause and prevent future flare-ups.

Collagen peptides have seemingly appeared out of nowhere. They are being advertised on social media, can be found on the covers of magazines… even my hairdresser has been talking about how she adds collagen peptides to her smoothie! But what are collagen peptides? Why is everyone adding this powder to their coffee, smoothies, or breakfast oatmeal bowl? And the real question is: Should you be adding collagen peptides to your diet as well?

Cellulite represents a localized skin concern typically found over the posterolateral thighs, buttocks, and abdomen. The skin surface over such areas is often found to exhibit dimpling or an “orange-peel” appearance

 Sweet almonds, when ingested, provide dietary fibre and healthy fats that are good for overall health and may be helpful for reducing cholesterol and decreasing the risk of coronary heart disease.
Sweet almonds, when ingested, provide dietary fibre and healthy fats that are good for overall health and may be helpful for reducing cholesterol and decreasing the risk of coronary heart disease.

 Dermatological conditions can often produce some of the most disturbing symptoms for patients to experience. They can be painful, itchy or release fluids, cause issues with self esteem and be constantly present as a reminder of an underlying condition.
Dermatological conditions can often produce some of the most disturbing symptoms for patients to experience. They can be painful, itchy or release fluids, cause issues with self esteem and be constantly present as a reminder of an underlying condition.
 Niacin is one form of vitamin B3. Niacinamide and inositol hexanicotinate are the other two forms of B3 that exist; these forms are generally used to treat different conditions within the body. B vitamins ultimately help the body utilize fats and proteins; they also help convert food into fuel which is then used to produce energy.
Niacin is one form of vitamin B3. Niacinamide and inositol hexanicotinate are the other two forms of B3 that exist; these forms are generally used to treat different conditions within the body. B vitamins ultimately help the body utilize fats and proteins; they also help convert food into fuel which is then used to produce energy.

 Noticing blood while brushing or flossing can be alarming and shouldn’t be ignored! The importance of oral health is a concept introduced to most Canadians at a very young age, and with good reason. The Ontario Dental Hygienist’s Association reports that the link between oral infections and other diseases in the body is becoming well-documented and accepted within the health-care community. Periodontal disease is one of the most common human diseases
Noticing blood while brushing or flossing can be alarming and shouldn’t be ignored! The importance of oral health is a concept introduced to most Canadians at a very young age, and with good reason. The Ontario Dental Hygienist’s Association reports that the link between oral infections and other diseases in the body is becoming well-documented and accepted within the health-care community. Periodontal disease is one of the most common human diseases
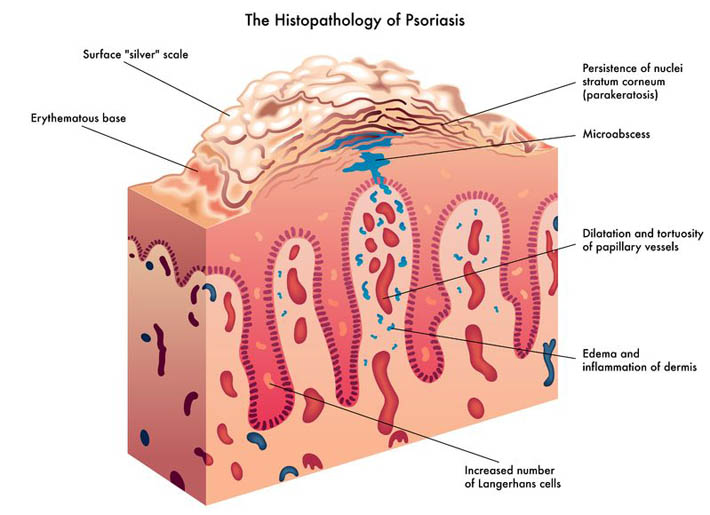
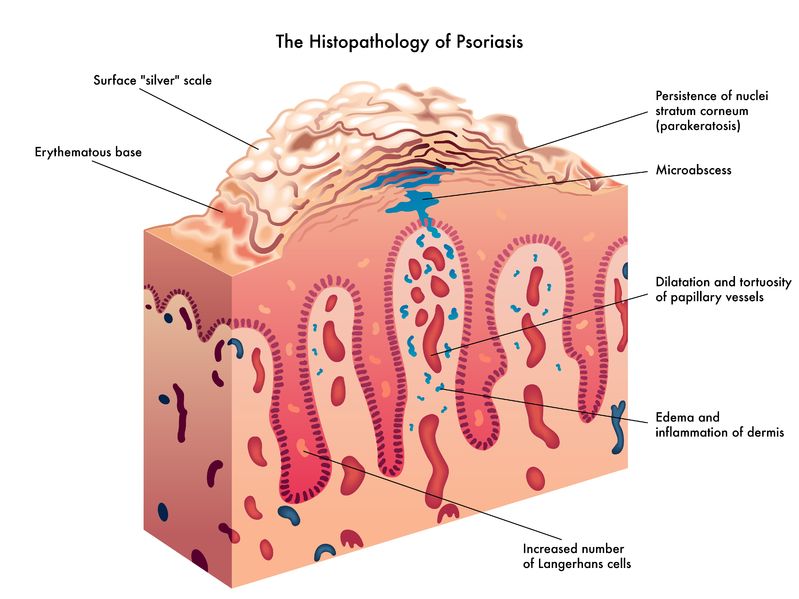 Psoriasis is a chronic skin condition that may have varying levels of symptom intensity. It causes skin cells to grow very quickly, which results in thick silvery or red patches of skin [1]. Usually, skin cells grow and turn over once a month and new skin grows to replace the old skin.
Psoriasis is a chronic skin condition that may have varying levels of symptom intensity. It causes skin cells to grow very quickly, which results in thick silvery or red patches of skin [1]. Usually, skin cells grow and turn over once a month and new skin grows to replace the old skin.

 Rosacea is a complex skin condition characterized by redness and flushing that could be transient or persistent.
Rosacea is a complex skin condition characterized by redness and flushing that could be transient or persistent.

 Periodontitis is the result of gingivitis progressing to a more serious stage. It is characterized by swollen, reddish, and bleeding gums, as well as bad breath. Severe periodontitis affects 10–15% of adults, while moderate periodontitis affects 40–60% of adults. Despite its high prevalence, it is largely unrepresented as a chronic inflammatory disease.
Periodontitis is the result of gingivitis progressing to a more serious stage. It is characterized by swollen, reddish, and bleeding gums, as well as bad breath. Severe periodontitis affects 10–15% of adults, while moderate periodontitis affects 40–60% of adults. Despite its high prevalence, it is largely unrepresented as a chronic inflammatory disease.

 Acne vulgaris is a skin condition that many people experience during their lifetime. Treatments that provide sustained results involve figuring out the root causes and treating the body from the inside out.
Acne vulgaris is a skin condition that many people experience during their lifetime. Treatments that provide sustained results involve figuring out the root causes and treating the body from the inside out.


Acne vulgaris is the most common dermatological issue seen by physicians. It is a condition that can cause a lot of distress, resulting in lowered self-esteem in some.

 And so it begins. You find few strands of hair on your pillow and more than the usual amount on your hair brush. As you are cleaning your house, you begin to notice hair on the floor, in the shower, on your clothes, and then it dawns on you that you are not only leaving behind a trail of hair in every area of the house, but a hairless patch possibly somewhere on your scalp.
And so it begins. You find few strands of hair on your pillow and more than the usual amount on your hair brush. As you are cleaning your house, you begin to notice hair on the floor, in the shower, on your clothes, and then it dawns on you that you are not only leaving behind a trail of hair in every area of the house, but a hairless patch possibly somewhere on your scalp.

Cleansers, toners, AM moisturizers, PM moisturizers, sunscreens, serums, gels, and ointments… With infomercials showcasing amazing before-and-after effects, and the daunting number of products lining cosmetics store shelves, acne can be challenging to manage. Is a regimen using a multitude of products necessary? What ingredients should be looked for if they are needed?
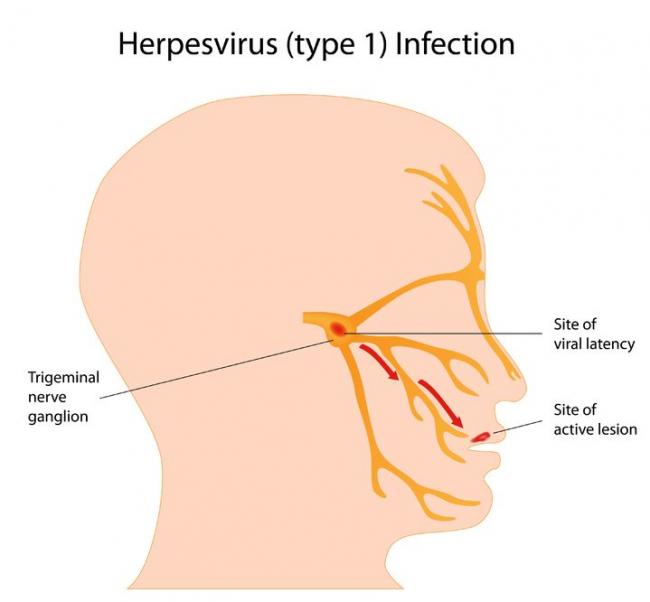
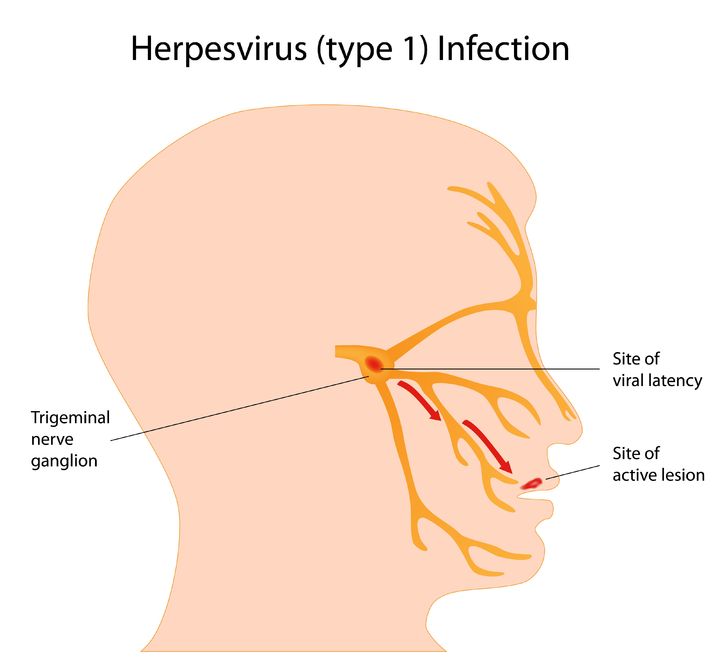 Herpes simplex virus (HSV) is a viral infection of the skin and mucous membranes. Lesions can occur in many different areas, especially in or around the mouth, lips, genitals, and eyes. There are two types of HSV that exist: HSV-1 and HSV-2. HSV-1 is responsible for the development of your typical “cold sore”; it therefore has a predisposition for the mouth and lips,
Herpes simplex virus (HSV) is a viral infection of the skin and mucous membranes. Lesions can occur in many different areas, especially in or around the mouth, lips, genitals, and eyes. There are two types of HSV that exist: HSV-1 and HSV-2. HSV-1 is responsible for the development of your typical “cold sore”; it therefore has a predisposition for the mouth and lips,

 We all do it. You know you’re guilty of it too. Want to know what I’m talking about? Personal hygiene. Do not get me wrong. This article is not going to tell you that personal hygiene is a bad thing, and shame on you for shampooing your hair and brushing your teeth.
We all do it. You know you’re guilty of it too. Want to know what I’m talking about? Personal hygiene. Do not get me wrong. This article is not going to tell you that personal hygiene is a bad thing, and shame on you for shampooing your hair and brushing your teeth.

 Who we are and how we feel is often expressed through our hair. Regardless of if hair is curly, straight, twisted, corn-rowed or locked; it is a universal sign of beauty, sensuality, fertility and attractiveness. Moreover, hair helps us to communicate our state of health. It also serves the function of protecting our heads and skin, adding not only a layer of insulation, but also more dimension to our personalities.
Who we are and how we feel is often expressed through our hair. Regardless of if hair is curly, straight, twisted, corn-rowed or locked; it is a universal sign of beauty, sensuality, fertility and attractiveness. Moreover, hair helps us to communicate our state of health. It also serves the function of protecting our heads and skin, adding not only a layer of insulation, but also more dimension to our personalities.

After iron, zinc is the most abundant element in the human body, with approximately 2 to 4 g distributed among the muscles (60%), bones (20%), liver, and skin. Given its abundance, concerns about zinc deficiency is often overlooked; however, as discussed in this article, certain populations and individuals may benefit from supplementation.