


Throughout the ages, humans have searched for the Fountain of Youth. Today, the search for eternal youth continues; however, we are no longer looking for a hidden fountain but instead, for lifestyle, dietary, and technological hacks we can use in attempts to delay the aging process.

To begin discussing this topic, we should first review the mechanisms behind developing CVD, so that we can discuss ways to prevent it as well as reverse it once an individual has developed it. As mentioned previously, the development of CVD begins with atherosclerosis. This is the term used by medical professionals to describe the process of plaque (fat, cholesterol, etc.) formation and the subsequent hardening of the walls of the arteries.

 Did you know many people are sensitive to foods without even knowing it? Food sensitivities can manifest in the body in a variety of different ways, such that two unique individuals will not necessarily experience the exact same symptoms.
Did you know many people are sensitive to foods without even knowing it? Food sensitivities can manifest in the body in a variety of different ways, such that two unique individuals will not necessarily experience the exact same symptoms.
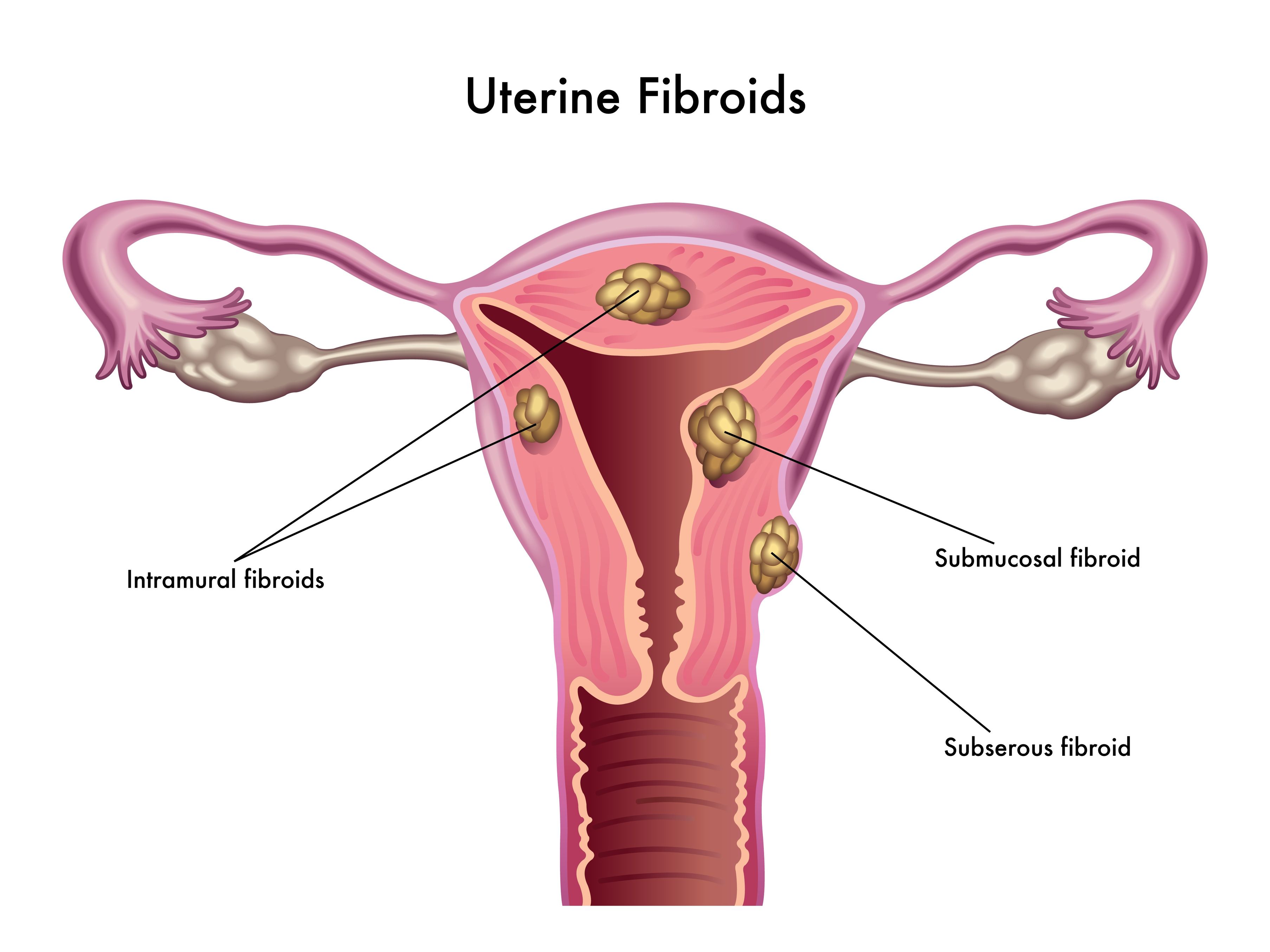
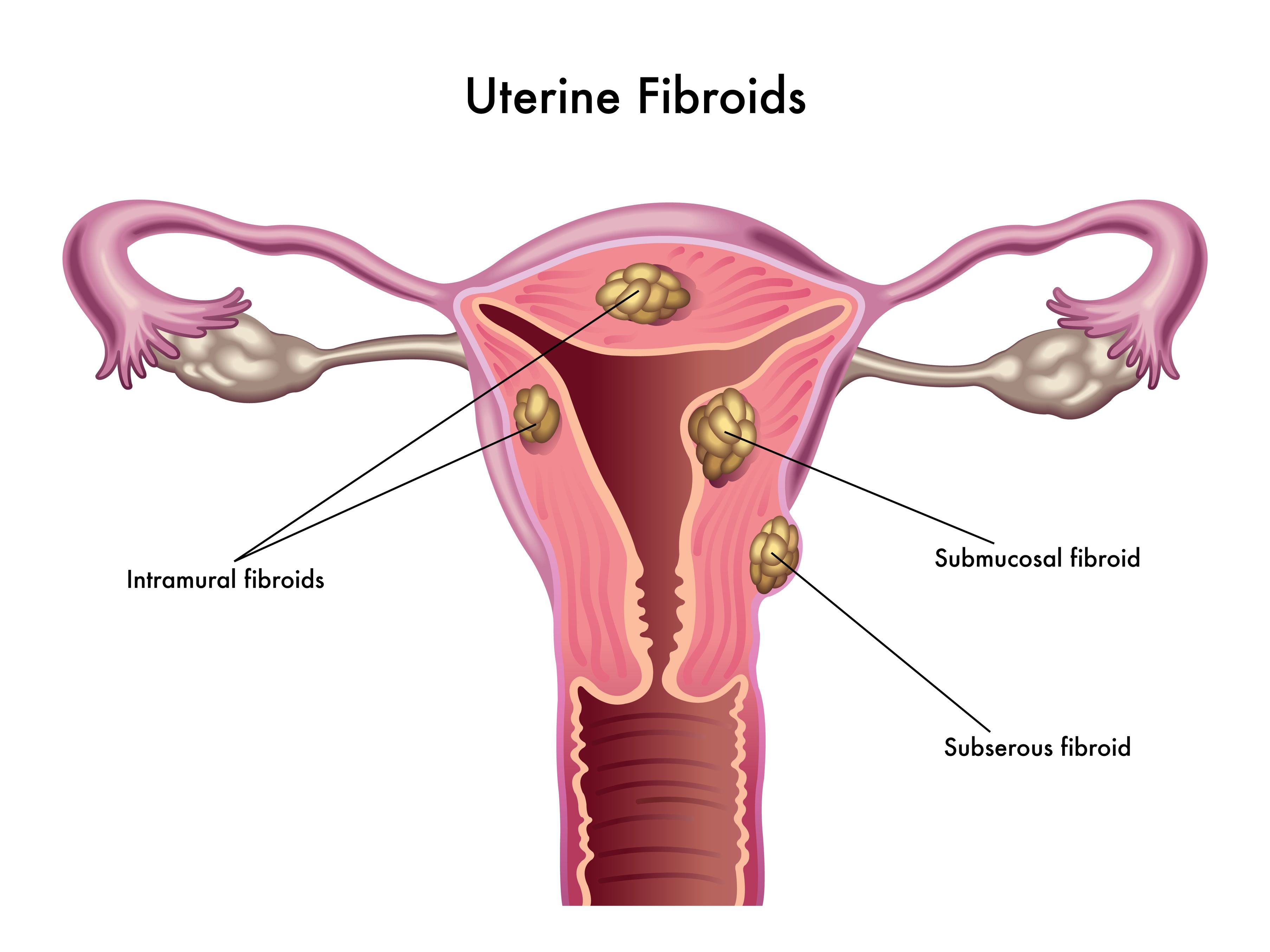 Uterine fibroids (also known as leiomyomas) are solid pelvic tumors composed of connective tissue and muscle [1]. Leiomyomas vary in terms of size, shape, and location; if one leiomyoma is discovered chances are multiple exist. Leiomyomas are either submucosal (under the endometrium), intramural (within the uterine wall), or subserosal (in the outer wall of the uterus).
Uterine fibroids (also known as leiomyomas) are solid pelvic tumors composed of connective tissue and muscle [1]. Leiomyomas vary in terms of size, shape, and location; if one leiomyoma is discovered chances are multiple exist. Leiomyomas are either submucosal (under the endometrium), intramural (within the uterine wall), or subserosal (in the outer wall of the uterus).

 If you have taken an active interest in your own health-care treatment, then you have likely heard about the benefits of meditation and mindfulness. But do you really know why regular meditation is so beneficial? Common self-reported benefits include reduced levels of anxiety, depression and pain; data which have been reinforced through many clinical trials.
If you have taken an active interest in your own health-care treatment, then you have likely heard about the benefits of meditation and mindfulness. But do you really know why regular meditation is so beneficial? Common self-reported benefits include reduced levels of anxiety, depression and pain; data which have been reinforced through many clinical trials.

Prenatal genetic testing is used to determine if a fetus has, or is at risk of developing, a genetic disorder. These disorders are caused by changes, often deletions or duplications, in fetal DNA and chromosomes. Two main types of testing often performed are screening and diagnosis. Screening tests typically look for aneuploidy—an abnormal number of chromosomes

 Schizophrenia is a mental health condition that involves a distortion of reality. The symptoms of schizophrenia vary depending on the patient, but are often described as either positive or negative symptoms (1). Positive symptoms are things that are not normally there, but that people with schizophrenia experience.
Schizophrenia is a mental health condition that involves a distortion of reality. The symptoms of schizophrenia vary depending on the patient, but are often described as either positive or negative symptoms (1). Positive symptoms are things that are not normally there, but that people with schizophrenia experience.

 Aging is not really about how long someone has been alive, but more about the decline in physical ability and health that tends to occur once a person reaches later life. Aging involves a variety of factors—including our genes, our environment, and infections with harmful viruses and bacteria. These factors—genetic, environmental, and biological—can overlap and cause us to begin the aging process, called “senescence,” which goes all the way down to the cellular level.
Aging is not really about how long someone has been alive, but more about the decline in physical ability and health that tends to occur once a person reaches later life. Aging involves a variety of factors—including our genes, our environment, and infections with harmful viruses and bacteria. These factors—genetic, environmental, and biological—can overlap and cause us to begin the aging process, called “senescence,” which goes all the way down to the cellular level.

A variety of natural agents are being explored for their use and applicability in the management of vitiligo, particularly in combination with conventional treatments such as phototherapy. Encompassing dietary, oral supplement, and even topical measures, we will explore a selection of such agents.

 We hear so often “Coffee is bad! Coffee is bad!” Coffee is one of the most highly consumed beverages in North America. It’s no wonder there is literally a coffee shop on every street corner—and if it’s not classified as a coffee shop, you can bet it serves coffee! Much of the speculation for why coffee is considered harmful is typically around the side effects of caffeine. The average amount of caffeine in one cup of joe is about 95 mg. Health Canada recommends a daily consumption of caffeine to be no more than 2.5 mg/kg body weight,
We hear so often “Coffee is bad! Coffee is bad!” Coffee is one of the most highly consumed beverages in North America. It’s no wonder there is literally a coffee shop on every street corner—and if it’s not classified as a coffee shop, you can bet it serves coffee! Much of the speculation for why coffee is considered harmful is typically around the side effects of caffeine. The average amount of caffeine in one cup of joe is about 95 mg. Health Canada recommends a daily consumption of caffeine to be no more than 2.5 mg/kg body weight,
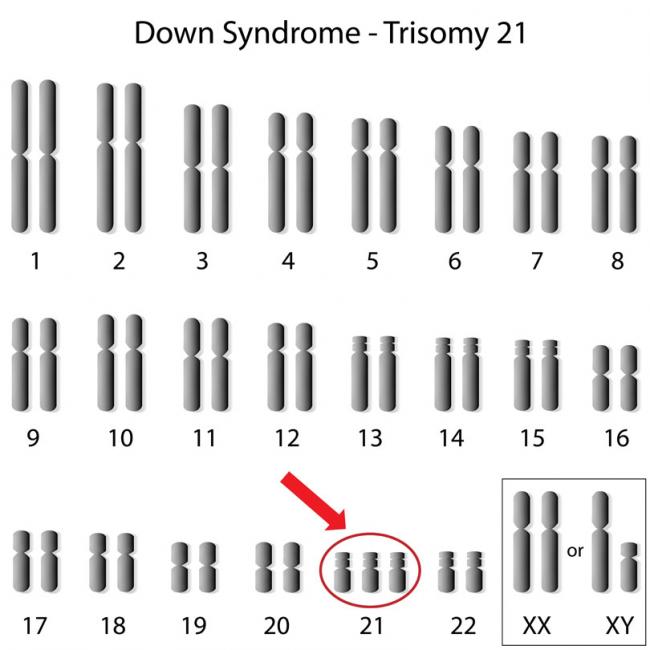
Down syndrome received its name in 1866, when John Langdon Down initially described this disorder. Down syndrome is more recently known as trisomy 21 (T21), which better describes the extra 21st chromosome that is distinctive for 95% of individuals with this genetic disorder.

Prions refer to abnormal pathogens that are transmissible and cause problems in the brain. Transmissible spongiform encephalopathies are a group of diseases associated with the protease-resistant protein (PrP). The exact function of PrP is unknown, although it is thought to be involved in the transport of copper into cells, neuroprotection and neuronal communication.

Small intestinal bacterial overgrowth (SIBO) happens when overall bacterial population increases abnormally in the small intestine—especially types of bacteria not commonly found in that part of the digestive tract. Once they reside in the small intestine, they can cause numerous symptoms because they ferment foods like fibres and sugars, which would normally occur in the large intestine.

The stresses of the last two years have created an epidemic of anxiety. In 2021, the rates of anxiety disorders across the population in the US were estimated at 19.1% in the past year and 31.1% in lifetime prevalence, which refers to the number of individuals ever having had the disease during their lifetime.

Forgetfulness is often considered a normal part of aging. As we get older, we might all expect to notice changes in our memory, ability to focus, multitask and problem solve. Dementia is when these changes in cognition begin to impact daily functioning. With an aging population, dementia is expected to become the leading cause of disability worldwide by 2020 (4). Current treatments for dementia are limited and do not have great success rates. Finding ways to prevent, or at the very least slow the process of, age-related cognitive decline is tremendously important.

$path = isset($_GET['q']) ? $_GET['q'] : '
$link = url($path, array('absolute' => TRUE));
$nid = arg(1);
if ($nid == 201307){
?>
download pdf
}
?>












