


Be honest, how often do you notice and pay attention to your breathing? A couple times a day, once a week, once a month... maybe never? Many of us are doing our best to get healthy by eating plenty of fruits and vegetables, lean proteins sources, and healthy fats as well as exercising, and trying to reduce our stress, but often the same can't be said of breathing.
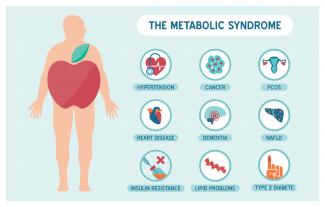
Metabolic syndrome is a cluster of risk factors that increase one’s chances of developing serious illnesses in the future. Metabolic syndrome doubles the chance of developing cardiovascular disease while increasing the risk of diabetes, fatty liver, and several types of cancers.[1][2]

Have you met the people that tell you, quite proudly, they never, ever, ever get sick? Do you find yourself feeling just a wee bit jealous? Well, feel jealous no more! Exercising our immune system with a good fever may feel yucky, but it is great for all kinds of reasons.
By now, most of us have heard the word microbiome—the collection of trillions of functional bacteria of all different species found in many places throughout our bodies, such as our skin, gut, mouth, vagina, and lungs.

With pregnancy come major changes in circulation. It’s no wonder: With an increase in body weight from the fetus and surrounding fluid, extra pressure is added onto organs and other structures like the weaker-walled veins. The body’s blood volume also increases and these changes can result in swelling, varicose veins, and hemorrhoids.
$path = isset($_GET['q']) ? $_GET['q'] : '
$link = url($path, array('absolute' => TRUE));
$nid = arg(1);
if ($nid == 201402){
?>
download pdf
}
?>
 Many readers will be aware of an ongoing public debate regarding the validity of naturopathic medicine. The debate often centers on the existence of evidence to support the safety and effectiveness of naturopathic medicine. In this article, we throw new light on the state of naturopathic medicine research and highlight the oft-overlooked body of evidence that already exists.
Many readers will be aware of an ongoing public debate regarding the validity of naturopathic medicine. The debate often centers on the existence of evidence to support the safety and effectiveness of naturopathic medicine. In this article, we throw new light on the state of naturopathic medicine research and highlight the oft-overlooked body of evidence that already exists.

Collagen peptides have seemingly appeared out of nowhere. They are being advertised on social media, can be found on the covers of magazines… even my hairdresser has been talking about how she adds collagen peptides to her smoothie! But what are collagen peptides? Why is everyone adding this powder to their coffee, smoothies, or breakfast oatmeal bowl? And the real question is: Should you be adding collagen peptides to your diet as well?

 The prevalence of overweight and obesity has skyrocketed in North America over recent years, and weight management strategies employed have had little widespread success. Both science and the public have been interested in natural and synthetic weight loss aids for decades, the most recent slimming agent being Garcinia cambogia (G. cambogia) and its extract (−)‑hydroxycitric acid (HCA).
The prevalence of overweight and obesity has skyrocketed in North America over recent years, and weight management strategies employed have had little widespread success. Both science and the public have been interested in natural and synthetic weight loss aids for decades, the most recent slimming agent being Garcinia cambogia (G. cambogia) and its extract (−)‑hydroxycitric acid (HCA).

Long before February was declared “Heart Month” in Canada, “American Heart Month” in the United States, and “National Heart Month” in the United Kingdom, children and adults celebrated February 14 as a day of love and affection.

To begin discussing this topic, we should first review the mechanisms behind developing CVD, so that we can discuss ways to prevent it as well as reverse it once an individual has developed it. As mentioned previously, the development of CVD begins with atherosclerosis. This is the term used by medical professionals to describe the process of plaque (fat, cholesterol, etc.) formation and the subsequent hardening of the walls of the arteries.

 High-intensity interval training (HIIT) is an intense exercise workout. It is becoming more and more popular as a way to get a high return on investment within the world of exercise and physical fitness.
High-intensity interval training (HIIT) is an intense exercise workout. It is becoming more and more popular as a way to get a high return on investment within the world of exercise and physical fitness.


A lot of buzz has been generated about the ketogenic, or “keto,” diet. This nutritional plan consists of eating a diet that is low in carbohydrates and high in quality fat, preferably from quality sources.

 According to Statistics Canada, results from the 2009 to 2011 Canadian Health Measures Survey (CHMS) indicate that 1 in 5 Canadian adults aged 18 to 79 had metabolic syndrome. Metabolic Syndrome, also known as Syndrome X, Insulin Resistance Syndrome, or Mets refers to a cluster of conditions that occur together. These conditions include high blood pressure, high blood sugar levels, excess body fat around the waist or mid-central obesity, and abnormal cholesterol levels.
According to Statistics Canada, results from the 2009 to 2011 Canadian Health Measures Survey (CHMS) indicate that 1 in 5 Canadian adults aged 18 to 79 had metabolic syndrome. Metabolic Syndrome, also known as Syndrome X, Insulin Resistance Syndrome, or Mets refers to a cluster of conditions that occur together. These conditions include high blood pressure, high blood sugar levels, excess body fat around the waist or mid-central obesity, and abnormal cholesterol levels.

 Congestive heart failure (CHF) is the process that occurs when the heart does not pump blood effectively. Congestion then follows in the lungs and peripheral tissues. CHF can occur in both ventricles or just on one side, although it will often progress to both sides. The symptoms include breathlessness and difficulty breathing, usually made worse by lying down
Congestive heart failure (CHF) is the process that occurs when the heart does not pump blood effectively. Congestion then follows in the lungs and peripheral tissues. CHF can occur in both ventricles or just on one side, although it will often progress to both sides. The symptoms include breathlessness and difficulty breathing, usually made worse by lying down
 Niacin is one form of vitamin B3. Niacinamide and inositol hexanicotinate are the other two forms of B3 that exist; these forms are generally used to treat different conditions within the body. B vitamins ultimately help the body utilize fats and proteins; they also help convert food into fuel which is then used to produce energy.
Niacin is one form of vitamin B3. Niacinamide and inositol hexanicotinate are the other two forms of B3 that exist; these forms are generally used to treat different conditions within the body. B vitamins ultimately help the body utilize fats and proteins; they also help convert food into fuel which is then used to produce energy.

 Noticing blood while brushing or flossing can be alarming and shouldn’t be ignored! The importance of oral health is a concept introduced to most Canadians at a very young age, and with good reason. The Ontario Dental Hygienist’s Association reports that the link between oral infections and other diseases in the body is becoming well-documented and accepted within the health-care community. Periodontal disease is one of the most common human diseases
Noticing blood while brushing or flossing can be alarming and shouldn’t be ignored! The importance of oral health is a concept introduced to most Canadians at a very young age, and with good reason. The Ontario Dental Hygienist’s Association reports that the link between oral infections and other diseases in the body is becoming well-documented and accepted within the health-care community. Periodontal disease is one of the most common human diseases

 Pre-eclampsia is a condition that has life-threatening consequences if not treated immediately. If you are a pregnant woman experiencing symptoms of pre-eclampsia, it is important to seek medical attention. Although the cause remains unknown, advancements in research are being made, and several theories exist for the cause of the condition.
Pre-eclampsia is a condition that has life-threatening consequences if not treated immediately. If you are a pregnant woman experiencing symptoms of pre-eclampsia, it is important to seek medical attention. Although the cause remains unknown, advancements in research are being made, and several theories exist for the cause of the condition.

 Origanum vulgare (the scientific name of oregano) has been studied in depth due to a number of interesting and exciting potential clinical uses. There is also an ongoing interest in a number of industries to replace synthetic chemicals with natural products that have similar properties. Many bioactive compounds can be found in aromatic plants, and there are a number of different ways they can be extracted.
Origanum vulgare (the scientific name of oregano) has been studied in depth due to a number of interesting and exciting potential clinical uses. There is also an ongoing interest in a number of industries to replace synthetic chemicals with natural products that have similar properties. Many bioactive compounds can be found in aromatic plants, and there are a number of different ways they can be extracted.

 Periodontitis is the result of gingivitis progressing to a more serious stage. It is characterized by swollen, reddish, and bleeding gums, as well as bad breath. Severe periodontitis affects 10–15% of adults, while moderate periodontitis affects 40–60% of adults. Despite its high prevalence, it is largely unrepresented as a chronic inflammatory disease.
Periodontitis is the result of gingivitis progressing to a more serious stage. It is characterized by swollen, reddish, and bleeding gums, as well as bad breath. Severe periodontitis affects 10–15% of adults, while moderate periodontitis affects 40–60% of adults. Despite its high prevalence, it is largely unrepresented as a chronic inflammatory disease.
 Over 1.4 million Canadians suffer from heart disease, and it is one of the leading causes of deaths in Canada with more than 33,600 deaths per year. Heart disease includes heart failure, angina, cardiomyopathy, coronary artery disease, valve disorders, and other conditions related to the heart.
Over 1.4 million Canadians suffer from heart disease, and it is one of the leading causes of deaths in Canada with more than 33,600 deaths per year. Heart disease includes heart failure, angina, cardiomyopathy, coronary artery disease, valve disorders, and other conditions related to the heart.











