


With pregnancy come major changes in circulation. It’s no wonder: With an increase in body weight from the fetus and surrounding fluid, extra pressure is added onto organs and other structures like the weaker-walled veins. The body’s blood volume also increases and these changes can result in swelling, varicose veins, and hemorrhoids.

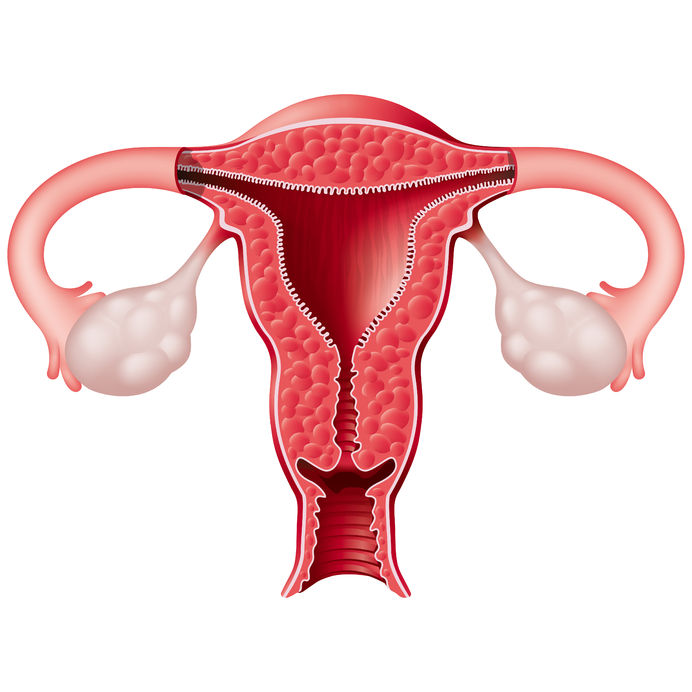
Polycystic ovarian syndrome (PCOS) is one of the most common endocrine disorders. PCOS affects one in every five women of the reproductive age.

Dies ist Teil 2 unseres zweiteiligen Artikels zu Möglichkeiten der Geburtenkontrolle neben der „Pille“.
Teil 1 behandelte die Hormon- und Kupferspiralen. Teil 2 deckt den Ring, das Pflaster, das Diaphragma, die Kondome und die Rhythmusmethode ab.

 There is a new, growing interest in the field of male infertility, given the recent trends of declining conception over the past decade. The times are telling of families having fewer children, later in age and often having more difficulties with conception. Infertility can pose physical, psychological, financial and economic burden on individuals, the health care system and society.
There is a new, growing interest in the field of male infertility, given the recent trends of declining conception over the past decade. The times are telling of families having fewer children, later in age and often having more difficulties with conception. Infertility can pose physical, psychological, financial and economic burden on individuals, the health care system and society.

 Male fertility is measured by sperm quality and count. A man is considered at risk for infertility if his sperm count is less than 20 million per millilitre, and may be sterile if the sperm count is less than 500,000 per millilitre. Semen analysis is commonly done by light microscope and scanning electron microscope. Female infertility has become a medical hot topic, but what about men; the other half of the equation?
Male fertility is measured by sperm quality and count. A man is considered at risk for infertility if his sperm count is less than 20 million per millilitre, and may be sterile if the sperm count is less than 500,000 per millilitre. Semen analysis is commonly done by light microscope and scanning electron microscope. Female infertility has become a medical hot topic, but what about men; the other half of the equation?

 Pre-eclampsia is a condition that has life-threatening consequences if not treated immediately. If you are a pregnant woman experiencing symptoms of pre-eclampsia, it is important to seek medical attention. Although the cause remains unknown, advancements in research are being made, and several theories exist for the cause of the condition.
Pre-eclampsia is a condition that has life-threatening consequences if not treated immediately. If you are a pregnant woman experiencing symptoms of pre-eclampsia, it is important to seek medical attention. Although the cause remains unknown, advancements in research are being made, and several theories exist for the cause of the condition.


You may have witnessed it either on tv or in reality; an emotionally labile woman, frantically scrounging for a tub of ice-cream or chocolate, snapping at any provoking comment regarding her behaviour around “that time of the month”.

 A common misconception that women have about their menstrual cycle is that the birth control pill (BCP) is prescribed to regulate their cycle; this couldn’t be further from the truth.
A common misconception that women have about their menstrual cycle is that the birth control pill (BCP) is prescribed to regulate their cycle; this couldn’t be further from the truth.


Fertility challenges associated with maternal aging are an ever-increasing concern and can add constant pressure and stress to females wanting to have children.


Is coffee part of your morning routine? Are you convinced that it is good for you? Have you ever considered that it might not be?

 Morning sickness, also known as nausea gravidarum, affects up to 80% of pregnant women. Nausea and vomiting are usually limited to the first seven to twelve weeks of pregnancy, but can go on for longer in some women.
Morning sickness, also known as nausea gravidarum, affects up to 80% of pregnant women. Nausea and vomiting are usually limited to the first seven to twelve weeks of pregnancy, but can go on for longer in some women.
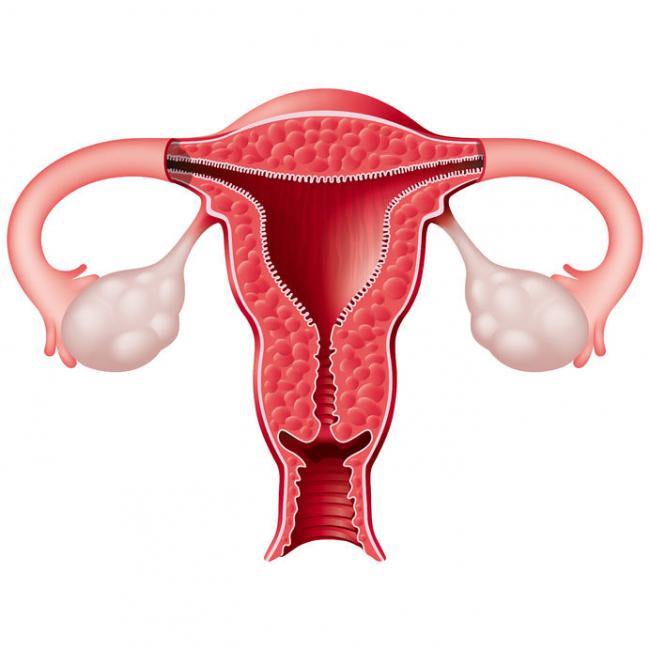
 Polycystic Ovary Syndrome (PCOS) is the most common cause of anovulatory infertility prevalent in 5-10% of women of reproductive age. Anovulation is abnormal ovarian function in which the ovary is unable to release an oocyte (egg) during a menstrual cycle
Polycystic Ovary Syndrome (PCOS) is the most common cause of anovulatory infertility prevalent in 5-10% of women of reproductive age. Anovulation is abnormal ovarian function in which the ovary is unable to release an oocyte (egg) during a menstrual cycle

Prenatal genetic testing is used to determine if a fetus has, or is at risk of developing, a genetic disorder. These disorders are caused by changes, often deletions or duplications, in fetal DNA and chromosomes. Two main types of testing often performed are screening and diagnosis. Screening tests typically look for aneuploidy—an abnormal number of chromosomes
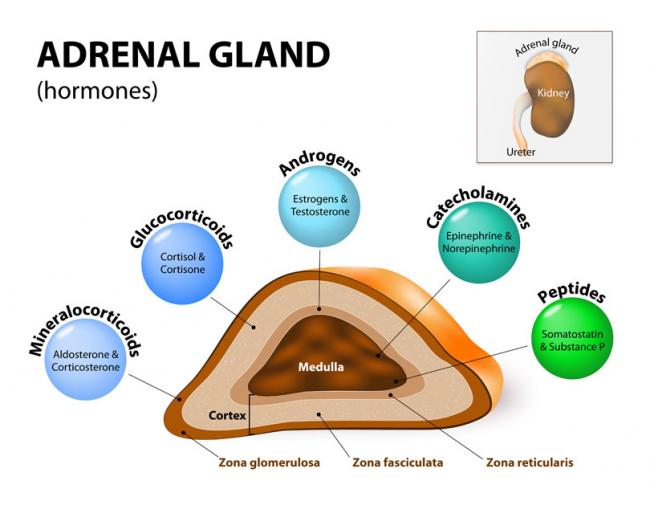
Stressed? In today’s world, we often hear about our adrenal glands being taxed and not performing optimally. Usually, we attribute this to external stressors such as work overload, emotional liabilities, relationship responsibilities, or financial strains. Have you ever thought this could be due to a genetic defect, though?
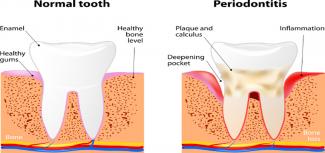
Sure, dental cleaning is great for our oral health, but did you know that it can also improve the wellness of your whole body? Daily toothbrushing and flossing is crucial to maintain the health of our gums and teeth; however, this might actually be more important in pregnant women and those looking to conceive.


OCP is one of the most-used forms of contraception in Canada, but more and more women are looking to alternatives to oral hormonal contraceptive methods.

 The joy of motherhood can be an exciting and blissful experience. But what if, instead of happiness and joy, the new mom is experiencing weepiness and irritation, and is crying all the time, but does not understand why? What if, instead of excitement at seeing her baby, she has negative feelings and worries that she may hurt her baby?
The joy of motherhood can be an exciting and blissful experience. But what if, instead of happiness and joy, the new mom is experiencing weepiness and irritation, and is crying all the time, but does not understand why? What if, instead of excitement at seeing her baby, she has negative feelings and worries that she may hurt her baby?

 The number of couples experiencing infertility and/or resorting to assisted reproductive technology (ART) is on the rise. A study released in 2012 found that among Canadian couples (women aged 18–44 years), the prevalence of infertility ranged from 11 to 15%, and this was an increase compared to previous statistics.
The number of couples experiencing infertility and/or resorting to assisted reproductive technology (ART) is on the rise. A study released in 2012 found that among Canadian couples (women aged 18–44 years), the prevalence of infertility ranged from 11 to 15%, and this was an increase compared to previous statistics. 
 Understanding your menstrual cycle involves more than just estimating your next period. Knowing your body and tracking your menstrual cycles can provide insight into your hormonal and reproductive health. You might be experiencing symptoms that we usually label as “normal,” when we should be calling them “common.”
Understanding your menstrual cycle involves more than just estimating your next period. Knowing your body and tracking your menstrual cycles can provide insight into your hormonal and reproductive health. You might be experiencing symptoms that we usually label as “normal,” when we should be calling them “common.”

 We all do it. You know you’re guilty of it too. Want to know what I’m talking about? Personal hygiene. Do not get me wrong. This article is not going to tell you that personal hygiene is a bad thing, and shame on you for shampooing your hair and brushing your teeth.
We all do it. You know you’re guilty of it too. Want to know what I’m talking about? Personal hygiene. Do not get me wrong. This article is not going to tell you that personal hygiene is a bad thing, and shame on you for shampooing your hair and brushing your teeth.










