Bone is our main structural support system. It allows us to protect our vital organs, facilitates movement, and creates a scaffold for blood vessels and nerves. In additional to the structural functions, bone has important metabolic and endocrine functions as well.

Collagen peptides have seemingly appeared out of nowhere. They are being advertised on social media, can be found on the covers of magazines… even my hairdresser has been talking about how she adds collagen peptides to her smoothie! But what are collagen peptides? Why is everyone adding this powder to their coffee, smoothies, or breakfast oatmeal bowl? And the real question is: Should you be adding collagen peptides to your diet as well?

 High-intensity interval training (HIIT) is an intense exercise workout. It is becoming more and more popular as a way to get a high return on investment within the world of exercise and physical fitness.
High-intensity interval training (HIIT) is an intense exercise workout. It is becoming more and more popular as a way to get a high return on investment within the world of exercise and physical fitness.

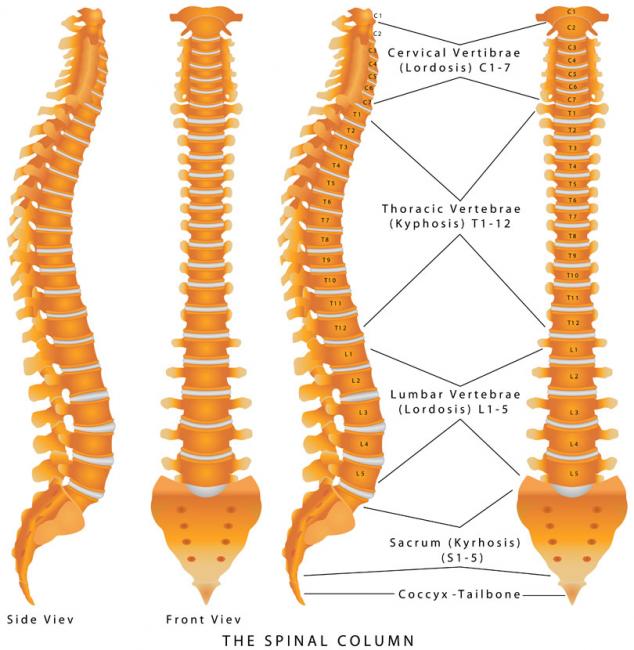
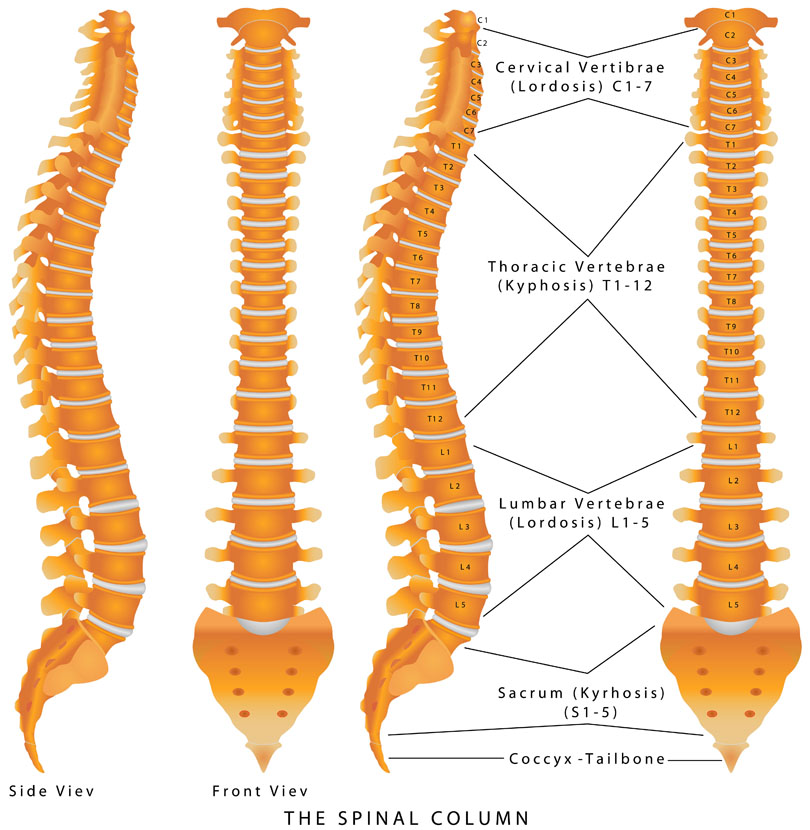
 Back pain is extremely common and has been experienced by almost everyone at one point in life. The official name for low back pain is lumbago, and it is literally defined as pain in the lower back. There are many possible causes for back pain, and often it is not even possible to identify a specific cause. If this is the case, it might be called nonspecific.
Back pain is extremely common and has been experienced by almost everyone at one point in life. The official name for low back pain is lumbago, and it is literally defined as pain in the lower back. There are many possible causes for back pain, and often it is not even possible to identify a specific cause. If this is the case, it might be called nonspecific.

 Whole-body cryotherapy (WBC) is a health promoting treatment that involves short exposures to air temperatures below −100°C [1]. WBC treatments last approximately 2-5 minutes and the frequency of treatments can vary based on the purpose of use. The patient is placed in a small cabin that emits a dry cold mist that is suctioned from a neighbouring liquid nitrogen tank.
Whole-body cryotherapy (WBC) is a health promoting treatment that involves short exposures to air temperatures below −100°C [1]. WBC treatments last approximately 2-5 minutes and the frequency of treatments can vary based on the purpose of use. The patient is placed in a small cabin that emits a dry cold mist that is suctioned from a neighbouring liquid nitrogen tank.

 Acute inflammation is something we want to get rid of so we can return to play and feel more comfortable. But inflammation has a purpose and a place in the short-term.
Acute inflammation is something we want to get rid of so we can return to play and feel more comfortable. But inflammation has a purpose and a place in the short-term.

 This action that berberine has on AMPK is one of the main reasons that interest in berberine’s effects on blood sugar management have been studied. AMPK activation is one the main mechanisms of action of the popular diabetes medication metformin (Glucophage). In human trials berberine has been extremely impressive in this regard. Let’s take a look at some of the studies.
This action that berberine has on AMPK is one of the main reasons that interest in berberine’s effects on blood sugar management have been studied. AMPK activation is one the main mechanisms of action of the popular diabetes medication metformin (Glucophage). In human trials berberine has been extremely impressive in this regard. Let’s take a look at some of the studies.

Chronic pain is a significant health issue, and it is estimated that one-half of those suffering with chronic pain have been suffering for longer than 10 years.[1] An estimated 54.4 million North Americans have been diagnosed with various arthritic disorders,[2] conditions that are typically treated with nonsteroidal anti-inflammatory drugs (NSAIDs).
 Walk down a busy street and you’ll see some atrocious body language and posture. Most people are hunched over, head down, eyebrows furrowed, and probably typing away on their cell phones. Anybody who is sitting is almost guaranteed to be hunched over: driving, eating, talking, on the phone, going to the toilet, working at a desk, studying, etc.
Walk down a busy street and you’ll see some atrocious body language and posture. Most people are hunched over, head down, eyebrows furrowed, and probably typing away on their cell phones. Anybody who is sitting is almost guaranteed to be hunched over: driving, eating, talking, on the phone, going to the toilet, working at a desk, studying, etc.
Have you ever injured yourself? Torn a ligament? Twisted an ankle? Separated a shoulder? If you weren’t healing and were experiencing inflammation, the likely treatment option offered by your medical doctor would be a cortisone injection.

Magnesium is the fourth most-abundant mineral in the human body, and is essential for the hundreds of metabolic and hormonal reactions occurring daily. It is generally known to be a component of bone formation (partnered with calcium), and is gaining more interest as a sleep aid due to its natural muscle relaxant properties.

 Many of us are aware that exercise is an important part of creating a healthy and balanced life. And yet, many more of us are so quick to create excuses and avoid the effort it takes to get our bodies moving. The truth of the matter is, there is no pill that can replicate what exercise can do for the human body. And like everything else that we do to occupy our time, if it is important enough to us, we will make it a priority. Exercise is an important part of managing every health concern, and here are three of my favourites.
Many of us are aware that exercise is an important part of creating a healthy and balanced life. And yet, many more of us are so quick to create excuses and avoid the effort it takes to get our bodies moving. The truth of the matter is, there is no pill that can replicate what exercise can do for the human body. And like everything else that we do to occupy our time, if it is important enough to us, we will make it a priority. Exercise is an important part of managing every health concern, and here are three of my favourites.

Protocols in naturopathic practice are designed to help increase health span while taking into consideration the extent of disease, a variety of modalities or tools of applicability, and patient choice and values; however, exercise prescriptions stand out as part of a foundational approach nearly ubiquitous and necessary for almost everyone.

$path = isset($_GET['q']) ? $_GET['q'] : '
$link = url($path, array('absolute' => TRUE));
$nid = arg(1);
if ($nid == 201401){
?>
download pdf
}
?>
 Turmeric is a golden-color spice widely used in South Eastern and Middle Eastern cooking. Besides being a popular spice, it is also an important herb used in many disciplines of medicine. The medicinal use of turmeric dates back to 4000 years ago in India. It takes on many different names: Indian saffron, haldi, rhizoma curcumae (jiang huang), asterre merite.
Turmeric is a golden-color spice widely used in South Eastern and Middle Eastern cooking. Besides being a popular spice, it is also an important herb used in many disciplines of medicine. The medicinal use of turmeric dates back to 4000 years ago in India. It takes on many different names: Indian saffron, haldi, rhizoma curcumae (jiang huang), asterre merite.

Acupuncture is a traditional therapy that has been used for thousands of years for the treatment of various ailments such as pain, fertility concerns, low energy, mood swings, and even colds and flu. It involves the insertion of very fine needles at specific points on the body to promote healing through the stimulation and circulation of “Qi.”

 Amyotrophic lateral sclerosis (ALS) is a neurodegenerative condition that affects the motor neurons of the cerebral cortex, brain stem, and spinal cord. It afflicts patients 55–75 years of age, and is slightly more common in men than women.
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative condition that affects the motor neurons of the cerebral cortex, brain stem, and spinal cord. It afflicts patients 55–75 years of age, and is slightly more common in men than women.
Amyotrophic lateral sclerosis (ALS), also known as Lou Gehrig’s disease, is a neuromuscular disease that is characterized by progressive nerve cell death leading to muscle weakness, paralysis and severe physical dysfunction. Approximately 2,500-3,000 Canadians currently live with this fatal disease.
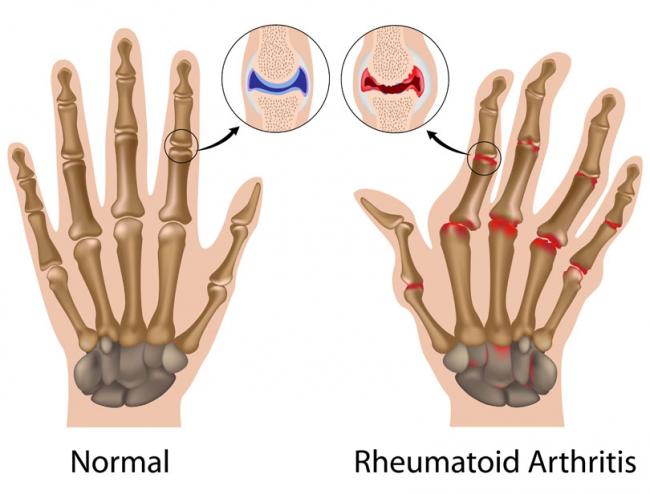
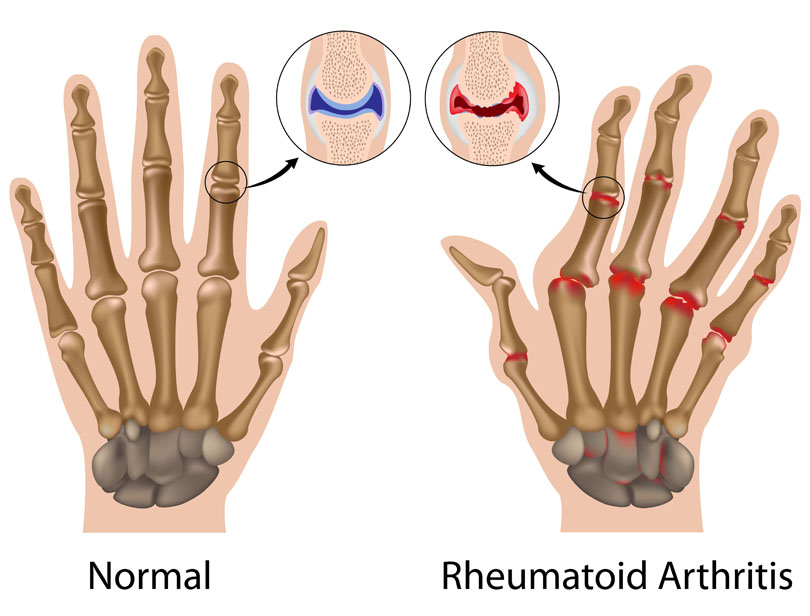 Rheumatoid arthritis (RA) is a chronic health condition that causes pain and stiffness in multiple joints, typically in the hands and feet. It impacts the lining of the joints, which, depending on the severity of the condition, causes pain, swelling, and deformity.
Rheumatoid arthritis (RA) is a chronic health condition that causes pain and stiffness in multiple joints, typically in the hands and feet. It impacts the lining of the joints, which, depending on the severity of the condition, causes pain, swelling, and deformity.

We know that exercise is good for us. It helps with our heart health, our blood sugar, our thyroid, our sleep, and our ability to manage stress. It helps with almost everything relating to our health and is probably one of the most important factors for good health, if not the most important.

Vitamin D3, also known as cholecalciferol or “the sunshine vitamin,” is an emerging nutrient with an array of potential therapeutic roles. In addition to its well-known role in bone health, vitamin D is being studied as an important agent in modulating immune function, mood, and cognitive function, as well as cardiovascular risk factors and protective effects against cancer development.