

The kidneys are one of the body’s most important filtration systems and are sometimes overlooked until there is an issue. In traditional Chinese medicine, the kidneys are often referred to as the “root of life,” and they play an important role in overall vitality, especially as we age.

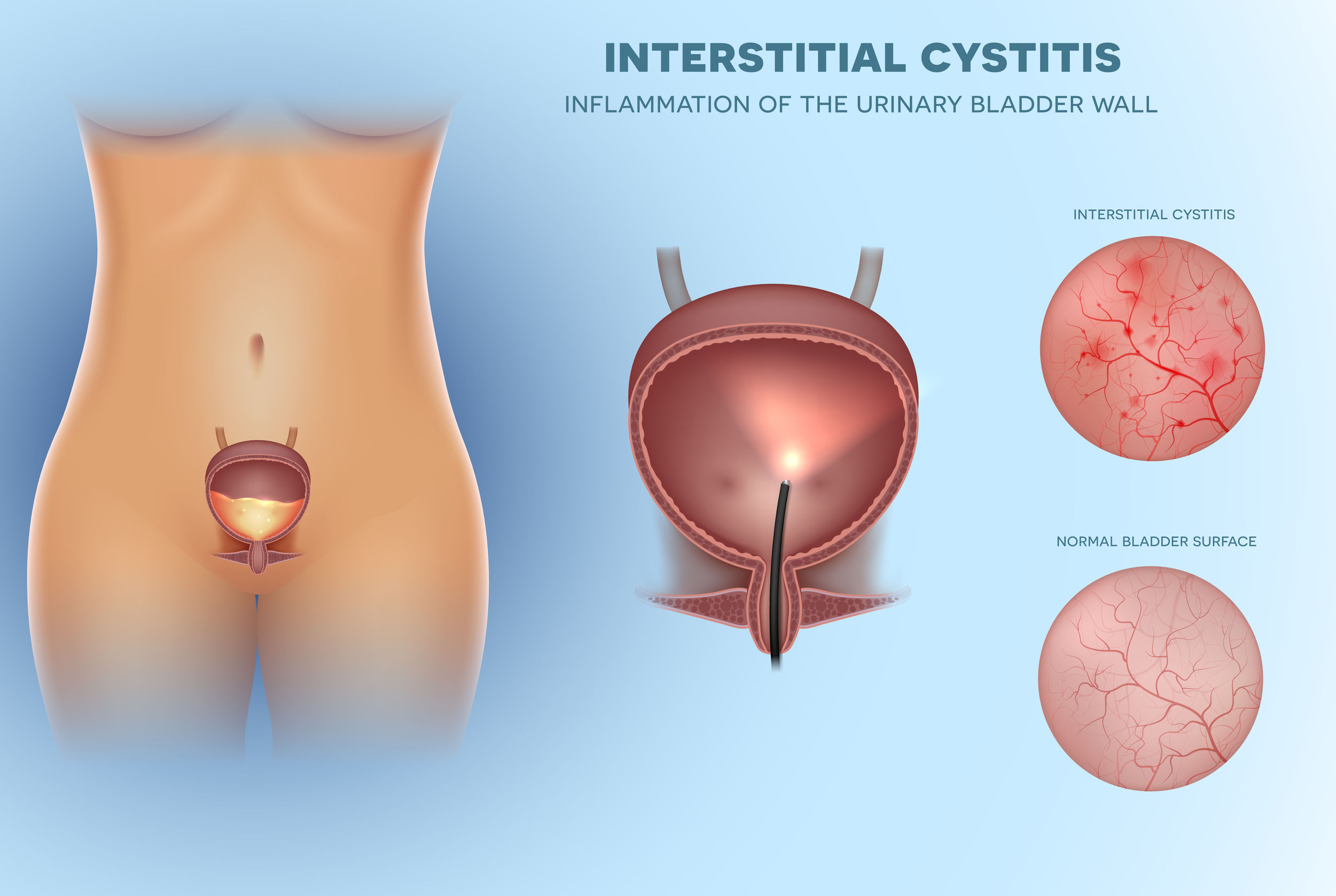
 Also known as bladder pain syndrome (BPS), IC is a chronic inflammatory condition that results in recurring discomfort or pain in the bladder and the surround pelvic region.
Also known as bladder pain syndrome (BPS), IC is a chronic inflammatory condition that results in recurring discomfort or pain in the bladder and the surround pelvic region.
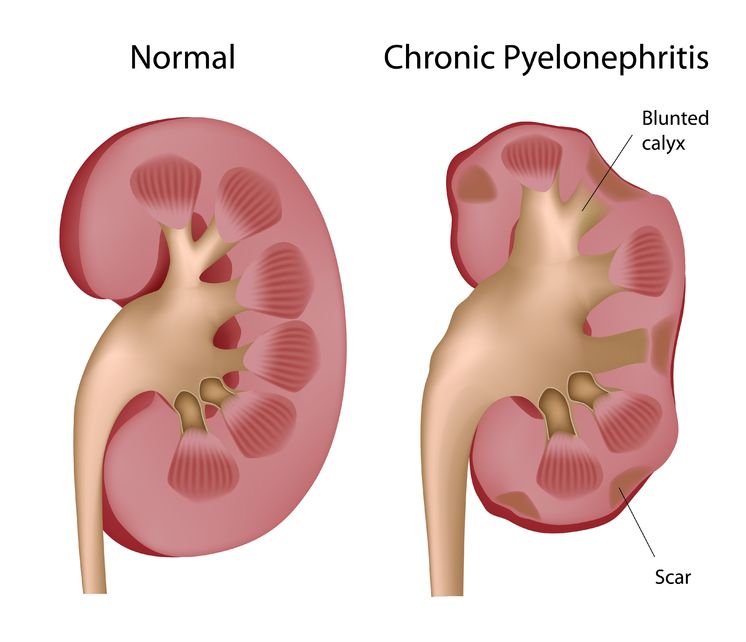
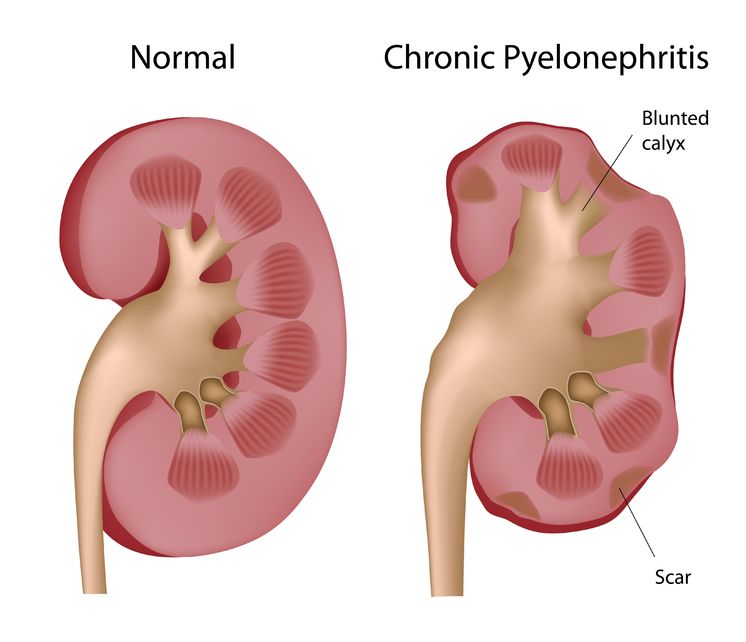 Pyelonephritis is the result of a progressive urinary tract infection, when a lower urinary infection travels upward into the upper urinary system. The lower urinary infections originate in the bladder and urethra, while the upper urinary infections involve the ureters and the kidneys. The kidneys filter the blood, so pyelonephritis can be potentially dangerous because an infection could then spread into the bloodstream.
Pyelonephritis is the result of a progressive urinary tract infection, when a lower urinary infection travels upward into the upper urinary system. The lower urinary infections originate in the bladder and urethra, while the upper urinary infections involve the ureters and the kidneys. The kidneys filter the blood, so pyelonephritis can be potentially dangerous because an infection could then spread into the bloodstream.

 Interstitial cystitis is a multifactorial condition and no single pathological process is present universally in patients with IC. It is thus important to determine the root causes of the individual’s symptoms, which commonly include bladder-wall dysfunction and permeability, urine acidity, and infection.
Interstitial cystitis is a multifactorial condition and no single pathological process is present universally in patients with IC. It is thus important to determine the root causes of the individual’s symptoms, which commonly include bladder-wall dysfunction and permeability, urine acidity, and infection.

Over 50% of women will suffer from a urinary tract infection (UTI) during their lifetime. One-third to one-half of these women will have a recurrent UTI within one year.

 Interstitial cystitis (IC) is a long-term disorder of the bladder. The exact cause of IC is unknown. The function of the bladder is to store urine that it receives from the kidneys. You can think of the bladder as acting like a balloon made of muscle. It expands to hold large amounts of urine, and contracts to squeeze it out.
Interstitial cystitis (IC) is a long-term disorder of the bladder. The exact cause of IC is unknown. The function of the bladder is to store urine that it receives from the kidneys. You can think of the bladder as acting like a balloon made of muscle. It expands to hold large amounts of urine, and contracts to squeeze it out.

 It is one of the first flowers to pop up in the spring. It can, quite quickly, become the bright, cheerful yellow that takes over a neatly manicured lawn. It is abundantly available and is usually easily recognized. Once it has planted itself, it can be very hard to remove.
It is one of the first flowers to pop up in the spring. It can, quite quickly, become the bright, cheerful yellow that takes over a neatly manicured lawn. It is abundantly available and is usually easily recognized. Once it has planted itself, it can be very hard to remove.
The urinary tract is part of the excretory system that removes wastes and unnecessary metabolites from the body to maintain homeostasis and biochemical balance. Made up of the kidneys, ureters, bladder, and urethra, the urinary tract is perceived to be sterile, except for the urethra.
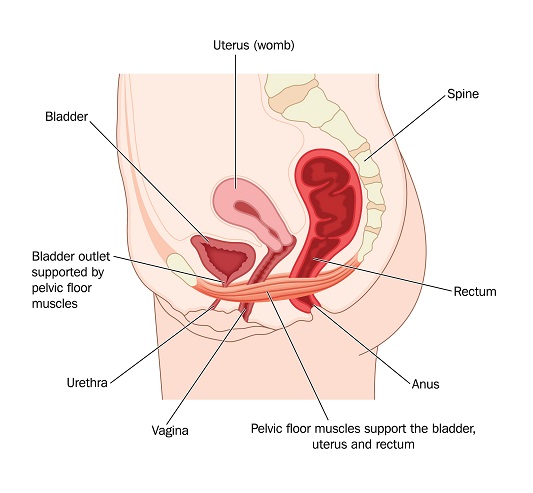
The structure of the pelvic floor creates a support system for the pelvic organs. These muscles, composed by the pelvic diaphragm and elevator ani complex, form a sling around the urethra, distal vagina, and rectum.

$path = isset($_GET['q']) ? $_GET['q'] : '
$link = url($path, array('absolute' => TRUE));
$nid = arg(1);
if ($nid == 201307){
?>
download pdf
}
?>